

The pulmonary circulation is made up of the blood vessels that carry oxygen-rich blood through the lungs (the pulmonary system). As the blood flows though the lungs, it loads up with oxygen and loses the carbon dioxide it is carrying. Then, the oxygen-rich blood returns to the heart through the left upper chamber (atrium), flows into the left lower chamber (ventricle) and out through the aorta to all cells in the body.
Once the oxygen is lost from the blood, the veins carry it back to the heart from all over the body. It flows into the heart’s right atrium. After the atrium is filled with blood, it squeezes (contracts) and sends the blood into the right ventricle. When the right ventricle fills and contracts, it pushes blood into the pulmonary artery. The pulmonary artery goes into the lungs through the pulmonary circulation.
A Pulmonary Thromboembolism refers to the clots that travel from veins in the body (emboli) and clog the arteries in the lungs. Once lodged in the lung arteries, they can cause more clots to form (thrombosis) and add more resistance to the blood flow through the lung.
This increased resistance from the clots increases the pressure inside the lungs. The medical term for increased pressure is hypertension. Combining these key words gives us the meaning of chronic thromboembolic pulmonary hypertension: High blood pressure in the pulmonary arteries that lasts six months or longer. The condition often happens after there is a pulmonary embolism.
Risk factors for PE and CTEPH
Risk factors for pulmonary embolism include:
The risk factors for developing CTEPH include:
What are the symptoms of CTEPH?
Many people who develop pulmonary hypertension after PE go through a so-called “honeymoon period” when they do not have any symptoms. When symptoms develop, they are vague and non-specific in the early stages of the disease. These include:
Symptoms of later-stage disease include fainting and signs of right heart failure, such as fluid retention (edema) and blue-tinged fingers and toes (cyanosis).
Some patients with CTEPH never have any early symptoms. Most times, the disease is discovered in these patients when they develop late-stage symptoms or during an autopsy.
How is CTEPH diagnosed?
If a physician suspects a patient has CTEPH, the next step is to perform imaging studies and specialized tests. These may include:
How is CTEPH treated?
A surgical procedure called a pulmonary thromboendarterectomy is currently the recommended and only effective treatment for patients with CTEPH. During this complex procedure, the surgeon cleans out the blockages in the pulmonary arteries in the right and left lungs using specialized tools. The surgery is performed through a chest incision while the patient’s heart is stopped. A heart-lung machine takes over the function of the heart and lungs during the procedure.
This surgery is considered a highly specialized procedure that should be performed only by an experienced team that includes cardiothoracic surgeons, anesthesiologists, perfusionists and intensivists at a medical center that has a successful track record with the procedure.
How well do patients do after the surgery?
When performed by an experienced team at a medical center with successful outcomes for this procedure, pulmonary thromboendarterectomy results in a complete cure in about 90 percent or more of patients. Success is measured by heart size and function and return of pulmonary blood pressure to normal limits. As surgical techniques and technology advance, outcomes continue to improve, and surgical mortality is now less than 3 percent.
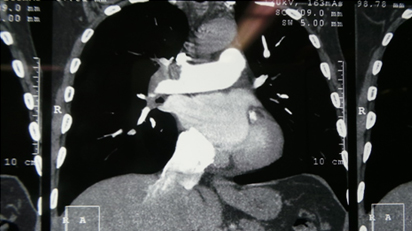
CT Pulmonary Angiography Showing Intra Pulmonary Filling defects
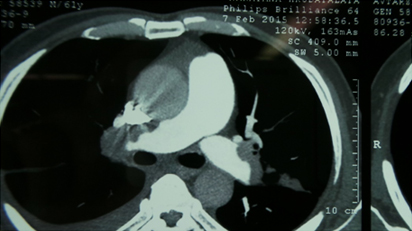
Filling Defects Within Pulmonary Artery
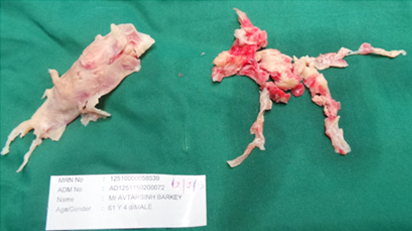
Operative Specimen of Chronic Pulmonary Thrombus